

Autism — also referred to as autism spectrum disorder (ASD), autism spectrum condition (ASC), or simply “being on the spectrum” — is a lifelong, highly heritable neurodevelopmental condition characterised by a brain that processes information more deeply and through fewer channels at once — producing differences in sensory experience, pattern recognition, social communication, and the need for predictability.
Autistic people are born autistic. Many autistic adults are identified late in life because their coping strategies, developed over decades without support, can mask the traits that assessors look for. Autism is not an intellectual disability, not a social deficit, and not something a person grows out of — it is what some autistic people describe as a different neurological operating system that has always been there.

Table of Contents[Hide][Show]
What is behind the autistic experience?
Where neurotypical brains tend to spread attention across many channels simultaneously, picking up the gist of everything, the autistic brain concentrates attention into fewer channels with more intensity, more detail, and more thoroughness per stream. This difference in how attention is distributed — described in the research literature as monotropism1 — shapes how autistic people experience sensory input, recognise patterns, navigate social situations, and regulate their internal world.
The result is a way of being in the world that differs from neurotypical experience in consistent, recognisable ways — but that has been so heavily filtered through clinical language and deficit framing that many autistic adults don’t recognise themselves in the descriptions they encounter. The goal of this entry is to describe what autism actually looks and feels like, from the inside, for adults who are encountering this information with the possibility that it might apply to them.
Autistic neurology
This deeper, less filtered style of processing is increasingly understood through neuroscience research into how autistic brains develop. Studies on synaptic pruning show that autistic brains retain more neural connections, particularly in the frontal, temporal, and parietal cortices2, producing a denser network that processes more thoroughly but is also more susceptible to overload.
For a fuller picture of how autistic neurology works at a structural level, see our entries on synaptic pruning and the mTOR pathway.
Autism is highly heritable — genetic factors account for the large majority of variance in autistic traits, making it one of the most strongly genetic neurodevelopmental conditions identified11. Autistic people are born autistic; it is not caused by parenting, environment, or anything that happens after birth.
A note on language
In many medical acronyms, the D stands for Disorder, Deficit, or Dysfunction. The shift from ASD to ASC (Autism Spectrum Condition) reflects a growing recognition that autism is a neurological difference, not an illness to be cured. You will encounter both terms in clinical and research contexts, and assessors may still use ASD because that is what appears in the diagnostic manuals.
Beyond the clinical terminology, autistic people describe themselves in a wide variety of ways: autistic, on the spectrum, Aspie, neurodivergent, or simply by their diagnostic label as it was given to them. Some prefer identity-first language (“autistic person”), others prefer person-first (“person with autism”), and both are valid. There is no single correct way to talk about your own neurology. However you choose to describe yourself — whether it’s the clinical term, the community term, or something else entirely — is the right one for you.
What autism looks and feels like in adults
The traits associated with autism are often described in clinical language that makes them sound like a checklist of deficits. In practice, the signs of autism in adults are better understood as a constellation of experiences that arise from the deep-processing style described above, each one shaping daily life in ways that can be both enriching and challenging. For many late-identified adults, learning about these experiences produces a feeling of sudden recognition — the sense that something about themselves has finally been named.
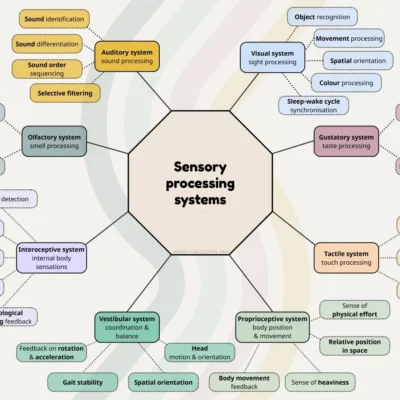

The sensory world
Autistic people typically experience sensory input with more intensity and less automatic filtering than neurotypical people. Sounds that others barely register can be physically painful. Textures, lighting, temperature, and smells can dominate awareness in a way that is difficult to explain to someone whose brain filters that input out automatically. This is not a sensitivity problem — it is the natural consequence of a nervous system that processes sensory data more thoroughly. Recent research has begun mapping exactly how this works through what researchers call “sticky” and “springy” attention12. Sticky attention — difficulty disengaging from whatever the brain is focused on — is associated with more intense sensory experiences, both pleasurable and aversive. Springy attention — a tendency to keep returning to a previous focus even after being pulled away — is associated with missing sensory information outside that focus. Together, these patterns help explain why the same autistic person can be overwhelmed by a sound that others barely notice and seem not to register something happening right next to them: the attention system is going deep, not wide, and what falls outside its beam may not get processed at all. When the environment cooperates (familiar textures, manageable sound levels, predictable lighting), the depth of sensory processing can be a source of genuine richness. When it doesn’t, the result is sensory overwhelm — a state of overload that affects cognition, emotion, and the ability to function.
Many autistic adults have spent decades managing their sensory environment without knowing that what they were doing had a name. Choosing specific fabrics, avoiding certain restaurants, always sitting in the same seat, wearing sunglasses indoors — these are not quirks. They are regulatory strategies built through years of trial and error. (For more on how this works, see our entries on sensory processing difficulties, hypersensitivity, and hyposensitivity.)
Patterns, detail, and information
One of the most consistent features of autistic cognition is an orientation toward patterns, systems, and connections. Autistic people often notice details that others miss, see relationships between ideas that others don’t connect, and find deep satisfaction in understanding how things fit together. The experience many autistic adults describe is something like “everything can be a puzzle” — a drive to figure out how things work, to trace causes back to their roots, and to build mental maps of how concepts interconnect.
This produces a particular relationship with information. Knowledge and clarity feel grounding — there is genuine comfort in understanding something thoroughly. Conversely, missing information, ambiguity, or situations where the relevant facts are not available can produce a visceral sense of being untethered. This is not simply a preference for detail. It is a processing style that relies on having enough data to build a coherent picture, and that becomes genuinely distressed when the data is insufficient. (This experience connects closely to intolerance of uncertainty, which has its own entry exploring the underlying mechanisms.)
The need for predictability and structure
Autistic brains invest heavily in predicting and mapping what will happen next. Routines, familiar environments, and predictable structures reduce cognitive load by providing a reliable framework that doesn’t need to be rebuilt from scratch every day. When autistic people plan ahead, create detailed contingency maps, or become distressed at unexpected changes, they are not being inflexible. They are managing a nervous system that processes change with more intensity and less automatic buffering than a neurotypical one.
This is often described clinically as “insistence on sameness” or as part of restricted repetitive behaviours — language that frames a functional coping strategy as a symptom. For most autistic adults, predictability is not a rigid need for control. It is what happens when a deeply processing brain tries to create enough structure to navigate a world that provides very little of it by default. (See our entries on intolerance of uncertainty, restricted repetitive behaviours, and rigid thinking for the fuller picture.)
Special interests
Autistic people often develop areas of deep, sustained engagement that go well beyond what is typically associated with hobbies. These special interests — sometimes called SPINs (SPecial INterests), intense interests, or passionate interests — are marked by a level of focus, emotional investment, and thoroughness that reflects the monotropic attention style. For many autistic adults, their interests are a primary source of joy, regulation, identity, and social connection.
Special interests are clinically categorised under restricted repetitive behaviours, a label that dramatically undersells what they actually are. The full picture — including how interests function, what happens when they’re suppressed, and why they matter so deeply — is explored in our dedicated special interests entry.
Stimming and self-regulation
Stimming — short for self-stimulatory behaviour — includes any repetitive movement, sound, or sensory input that serves a regulatory function. Rocking, hand-flapping, humming, tapping, chewing, spinning objects, repeating phrases — these are all ways the body manages the intensity of a deeply processing nervous system. Stimming can serve to calm, to focus, to express emotion, or simply to feel good.
Many autistic adults were taught, explicitly or implicitly, that their stims were unacceptable. The result is a lifetime of suppression that adds another layer of cognitive load to an already demanding day. Some people don’t recognise their own stims because they’ve been masked for so long — the movements have been made smaller, the sounds have been internalised, the impulse has been redirected into something less visible. Conscious unmasking sometimes reveals stims that were always there underneath, waiting to be allowed. (For more, see our entries on stimming, echolalia, and masking.)
Social communication
Autistic people process and express social information differently from neurotypical people. This is often described clinically as a social communication deficit, but that framing tells less than half the story. The fuller picture is explored in a dedicated section below — The social world: mismatch, not deficit.
Why so many autistic adults are identified late
If autism is lifelong and present from early development, why do so many people reach their thirties, forties, or fifties without knowing? Late autism diagnosis is increasingly common — not because autism is becoming more prevalent, but because recognition is finally catching up. The answer involves several interlocking factors, most of which have nothing to do with the person and everything to do with how the diagnostic system was built.
The criteria were designed around children
The diagnostic criteria for autism were developed primarily through observation of children, and overwhelmingly through observation of boys. The first formal inclusion of autism in diagnostic manuals (DSM-III, 1980) restricted the diagnosis to children under 30 months.
It was not until DSM-5 in 2013 that autism was formally recognised as a lifelong condition — a change driven in significant part by autistic advocates, including Ari Ne’eman and Steven Kapp, during the DSM consultation process. And it was in the DSM-5-TR in 2022 — four years ago — that the diagnostic manual first acknowledged that autism can present differently in women and that camouflaging behaviours exist.3
The ICD-11, updated in the same year, still lacks clear gender differentiation. This means that the tools and frameworks many clinicians use were built from research that systematically excluded the very people now seeking diagnosis: adults, women, and anyone whose autism doesn’t match the stereotypical presentation.
Autism is diagnostically characterised by challenges in social interaction, communication, and repetitive or restrictive behaviours. However, many of the traits included in the diagnostic criteria are often simply how an autistic person experiences distress when their needs are not met, and they are not supported by adaptations.
Women are disproportionately missed and misdiagnosed
Autistic women and gender-diverse people are frequently diagnosed years or even decades later than autistic men, often only after their existing coping strategies break down under increased life demands. Research shows that 65.8% of autistic women received a prior psychiatric diagnosis — most commonly anxiety, depression, borderline personality disorder, eating disorders, or OCD — before autism was considered, compared to 34.2% of men3. These earlier diagnoses are not always wrong (co-occurring conditions are common), but they can function as diagnostic overshadowing: the clinician sees the anxiety or the depression and stops looking for what’s underneath it.
The reasons for this gap are structural. Autistic women tend to develop more sophisticated masking and compensation strategies, often from a very young age. They may have special interests that appear “socially acceptable” (people, psychology, animals, literature) rather than stereotypically autistic. Their social difficulties may present as exhaustion and burnout rather than visible awkwardness. And the screening tools most commonly used in assessment were developed and validated primarily on male presentations, meaning they are measurably less sensitive to how autism looks in women3.
The masking paradox
Many autistic adults who reached adulthood without identification did so because they developed elaborate survival strategies. They learned social scripts, studied other people’s behaviour, rehearsed conversations, found ways to manage or hide sensory distress, and built routines that kept them functional. This was not a conscious choice to deceive — it was adaptation, developed under pressure, often in response to punishment or social rejection that started in early childhood. A child who is bullied for flapping their hands learns to sit on them. A teenager who is mocked for their intense interests learns to stop talking about them. An adult who has been told their whole life that they’re “too much” or “too sensitive” learns to perform a version of themselves that other people find acceptable.
The cruelty of this adaptation is that it is then used as evidence against the person. “You don’t look autistic” is one of the most common responses adults receive when they disclose or seek assessment. What that statement actually reflects is decades of exhausting, invisible labour — a person who has been managing a neurological difference without support, at enormous personal cost, and doing it well enough that the effort has become invisible to everyone around them. The very skills that kept them safe now function as barriers to identification and support.
Autism and intellectual disability
One of the most persistent misconceptions about autism is that it implies intellectual disability. This association exists because of how the diagnosis was historically applied. Leo Kanner’s original description of autism in the 1940s focused on children who had both autistic traits and significant intellectual disabilities. When Hans Asperger described children with similar social and behavioural patterns but without intellectual disability, a separate diagnostic label — Asperger’s syndrome — was created to distinguish them. For decades, “autism” in clinical practice effectively meant autism plus intellectual disability, and “Asperger’s” meant autism without it.
Since DSM-5 in 2013, both are understood as part of the same spectrum, and the current diagnostic framework uses specifiers (such as “with or without intellectual impairment”) rather than separate labels. The research is straightforward on this: most autistic adults do not have intellectual disabilities413, though autism is more prevalent among people who do. Intelligence is not a barrier to being autistic, and being articulate, educated, or professionally successful does not make someone less autistic — it means their autism has been expressed and managed in ways that happen to align with what society rewards.
Some people still use the term Asperger’s, particularly those who were diagnosed under that label before the change. That is a personal choice to be respected. Diagnostic categories evolve, but a person’s relationship to their own diagnosis belongs to them.
The social world: mismatch, not deficit
The social dimension of autism is the one most heavily distorted by clinical framing. Diagnostic criteria describe “deficits in social communication and social interaction,” which implies that autistic people lack social ability. The research tells a more complicated and much more interesting story.
How neurotypical social knowledge is built
Neurotypical people don’t get explicitly taught most social rules. Instead, they absorb them implicitly, starting in infancy, through a fast, unconscious process of observation and feedback. Research shows that by eleven months, infants are already linking conformity to positive social evaluation. By age three, children infer general rules from a single observation and enforce them on others, even when no adult has stated a rule exists5. This implicit learning runs constantly in the background, processing faces, tone, body language, and group dynamics simultaneously, and by adulthood, it has become so thoroughly internalised that most neurotypical people cannot articulate the rules they’re following. The knowledge doesn’t feel like knowledge anymore — it feels like intuition, like “just knowing” how things work.
A different pathway to social understanding
The autistic brain doesn’t run this background acquisition process in the same way. The monotropic attention style — deep and focused rather than broad and diffuse — means that the passive, simultaneous absorption of social data that neurotypical development relies on doesn’t happen automatically. Autistic people still learn social rules, but through a different pathway: conscious observation, deliberate analysis, working backwards from outcomes to figure out what the rule must have been.
The experience many autistic adults describe is the feeling that everyone else was given instructions they never received. That is, in a sense, accurate — not because the instructions were withheld, but because the delivery method (implicit, automatic, unconscious) is one that the autistic brain doesn’t prioritise. The explicit pathway works well, sometimes exceptionally well. Many late-identified autistic adults are highly socially skilled precisely because they’ve been consciously studying social dynamics for decades. But conscious processing never becomes fully automatic the way a first language does. It always costs more effort. Every interaction involves running the social translation in real time, which is cognitively demanding in a way that is invisible to everyone watching.
The experience has something in common with learning a second language as an adult. You can become completely fluent — grammar, vocabulary, idioms, humour — but you had to learn it all explicitly, and certain things that native speakers absorb without thinking (when “how are you?” is a real question versus a greeting, for instance, or the precise social weight of different ways of saying “no”) require conscious study. The fluency is real, but the path to it was different, and it never stops requiring a little more cognitive work than it does for someone who grew up inside that language.
A 2023 study by De Felice and colleagues demonstrated this distinction directly: autistic and neurotypical adults learned equally well in live, interactive teaching sessions, enjoyed them equally, and reported similar anxiety levels6. The researchers proposed a distinction between learning about social information (reading faces, interpreting tone — the implicit channel) and learning via social interaction (using social exchange as a medium for acquiring knowledge, which works equally well for both groups). Social interaction as a way of connecting and exchanging information is not the problem. The specific channel through which social rules are implicitly acquired is where the difference lies.
The bias runs both ways
Research on first impressions has revealed something important about whose “difficulty” this actually is. In a series of studies, Sasson and colleagues found that neurotypical observers formed significantly less favourable impressions of autistic adults within seconds of seeing them — rating them as more awkward, less likeable, and less approachable — and were less willing to pursue social interaction with them7. These judgments were remarkably stable, did not improve with increased exposure, and persisted across both child and adult age groups.

But when the same observers could only read transcripts of the conversations — removing all audiovisual cues — the bias disappeared entirely. The conversational content was equivalent. The rejection was based on differences in gaze patterns, facial expressivity, and vocal prosody: style, not substance.
A follow-up study found that these negative first impressions improved significantly when observers were told the person was autistic, and improved even further when the observers had greater autism knowledge8. It was specifically understanding — not intelligence, not age, not the observer’s own neurodivergent traits — that reduced the bias. This suggests that a significant portion of the social difficulty attributed to autistic people is actually a knowledge gap on the part of the people around them.
Autistic people connect well with each other
Perhaps the most telling evidence against the “social deficit” narrative comes from research on autistic-to-autistic interaction. A study by Heasman and Gillespie observed autistic adults interacting during collaborative activities and identified two distinctive features of what they termed neurodivergent intersubjectivity9. The first was a generous assumption of common ground — participants would make bold, specific references to shared cultural knowledge (quoting films, referencing game lore, dropping into character voices) without signalling or checking for understanding first. When the other person shared that reference point, it produced rapid rapport and a creative, joyful exchange. When they didn’t, the moment simply passed without distress. The second feature was a low demand for coordination — conversations could run in parallel tracks, drift apart and come back together, without this being experienced as a failure of communication. Both features are things that neurotypical social norms would flag as “atypical” or “disconnected,” but within the autistic group, they were functional, flexible, and often produced richer interaction than tightly coordinated neurotypical-style turn-taking would have.
This body of research collectively supports what autistic researcher Damian Milton named the double empathy problem in 2012. Social difficulties between autistic and neurotypical people are not caused by an autistic deficit, but by a mutual mismatch between two different communication systems. Each system works well internally. The friction arises at the interface between them, and the responsibility for bridging that gap should not fall on the autistic person alone. (See our full entry on double empathy for more.)
The disabling aspects of autism can be greatly reduced by accommodations, adjustments, and creating a more accessible and less ableist society.
The terminology and history of autism
Autism has been defined and redefined repeatedly over the past eight decades, and the language used to describe it is still evolving. If you’ve recently been assessed, received a diagnosis, or started reading about autism for the first time, you’ll encounter a range of terms — some current, some outdated, some actively contested. Here’s how the terminology has shifted and what the labels mean.
A brief timeline
- 1925 — Soviet child psychiatrist Grunya Sukhareva publishes the earliest known clinical description of autistic traits, based on her work with six children at a Moscow clinic. Her account is notably nuanced and non-pathologising for its era, describing a distinct cognitive style rather than a defect. Her work is published in German but is largely ignored by Western psychiatry for the next seven decades — partly due to misogyny, partly due to the Cold War isolation of Soviet science, and partly because Kanner (who read German) never credits her. Sula Wolff translated the 1925 paper into English in 1996, and Sukhareva’s priority began to be formally acknowledged in autism scholarship from the 2010s onwards.
- 1943 — Leo Kanner publishes his description of “early infantile autism” in English, focused on children with significant support needs and intellectual disabilities. Kanner’s work — not Sukhareva’s — becomes the foundational reference for autism in the English-speaking world, and shapes the diagnostic criteria for the next several decades.
- 1944 — Hans Asperger describes children with similar social and behavioural patterns but without intellectual disability, though his work doesn’t reach English-language audiences until decades later.
- 1980 — DSM-III introduces “Infantile Autism” as a formal diagnosis, restricted to children under 30 months. Male-centred criteria; no acknowledgement of how autism might present across genders.
- 1994 — DSM-IV introduces Asperger’s Disorder as a separate diagnosis alongside Autistic Disorder and PDD-NOS (Pervasive Developmental Disorder — Not Otherwise Specified).
- 2013 — DSM-5 removes the separate categories, combining everything under Autism Spectrum Disorder (ASD) with severity levels and specifiers. Recognises autism as lifelong.
- 2022 — DSM-5-TR includes the first acknowledgement of female-specific phenotypes and camouflaging behaviours. ICD-11 aligns with the spectrum model but still lacks gender differentiation.
What are the DSM and the ICD?
Two diagnostic systems shape how autism is defined and assessed around the world.
The DSM (Diagnostic and Statistical Manual of Mental Disorders), published by the American Psychiatric Association, is the primary framework used in the United States, Canada, and much of the English-speaking world.
The ICD (International Classification of Diseases), maintained by the World Health Organisation, is used more widely across Europe, Asia, and in global public health contexts, including the NHS in the UK.
In practice, many clinicians are familiar with both, and the two systems have increasingly aligned — but they don’t always update at the same pace, and a diagnosis made under one system may use different terminology or criteria than the other. If you’ve been assessed, the language in your report will reflect whichever system your assessor used, which in turn depends partly on where in the world you were assessed.
Asperger’s syndrome
The separate Asperger’s diagnosis no longer exists in current diagnostic manuals, but the term remains in wide use. Many adults were diagnosed under that label, and it appears in their documentation, their sense of identity, and the language they use about themselves. Not every country uses the DSM, and some clinical frameworks still use Asperger’s or equivalent terms.
Understood in historical context, what Kanner called autism was what we would now describe as autism with co-occurring intellectual disability. What Asperger described was autism without intellectual disability. The current understanding is that these are not different conditions — they are the same neurological profile with varying levels of co-occurring features and support needs.
Functioning labels
You may encounter the terms “high-functioning” and “low-functioning” autism. These terms are widely opposed within the autistic community because they describe how visible or convenient a person’s autism is to the people around them, rather than what the person actually experiences. “High-functioning” tends to mean “your struggles are invisible, so we won’t support you.” “Low-functioning” tends to mean “your strengths are invisible, so we won’t expect anything of you.” Neither reflects the person’s internal reality. The DSM-5 uses support levels (1, 2, and 3), which are an improvement but still describe external presentation rather than internal experience.
Spectrum — what it actually means
“The spectrum” is widely misunderstood. The most common misconception is that it’s a line from “a little bit autistic” to “very autistic.” A further extension of this thinking is the idea that everyone is somewhere on the spectrum, with “not autistic” at one end and “very autistic” at the other — which effectively reframes autism as a personality trait that everyone has to some degree.
That is not what the spectrum means.
Autism is a distinct neurological profile. You either have it, or you don’t, in the same way that you either have red hair or you don’t — there isn’t a spectrum of “a bit red-haired.” What varies is how autism presents, which traits are most prominent, and how much support a person needs in different areas of life. An autistic person might have very high support needs in sensory environments but none in intellectual tasks, or struggle significantly with social communication but thrive in structured work.
The spectrum describes that range and combination, not a single scale of severity that fades into neurotypicality at one end. A more accurate image than a line is what the neurodivergent community calls a spiky profile — a chart with many dimensions (sensory processing, social communication, executive function, language, motor skills, and so on) where each person’s scores spike high in some areas and dip low in others. The shape of the profile is different for every autistic person, which is why no two autistic people look the same from the outside, even though the underlying neurology is recognisably shared.
Co-occurring conditions and AuDHD
Autism frequently co-occurs with other conditions — not because autism causes them, but because the same underlying neurological differences that produce autistic traits also increase the likelihood of certain other presentations.
The most significant overlap is with ADHD. Research suggests that 40-60% of autistic children also meet the criteria for ADHD, and the overlap in adults — while less extensively studied — is increasingly recognised10. This combination is commonly known as AuDHD. Until DSM-5 in 2013, a dual diagnosis of autism and ADHD was not permitted, meaning many people with both were identified with only one (if either). (See our full AuDHD entry for more on how the two interact.)
Other commonly co-occurring conditions include anxiety disorders, depression, OCD, PTSD, eating difficulties (including ARFID), sleep disorders, sensory processing disorder, and specific learning difficulties, including dyslexia, dyspraxia, dysgraphia, and dyscalculia. The high rate of co-occurring anxiety and depression in autistic adults is partly attributable to the sustained cognitive and emotional cost of navigating a world that was not designed with autistic processing in mind — a cost that compounds over a lifetime, particularly when the person doesn’t know why everything feels so much harder.
An observation: regulation and distribution
One way to think about the relationship between autism and ADHD is through the lens of attention.
In ADHD, attention is regulated differently — the system that decides when attention engages and disengages is interest-based rather than priority-based, driven by the dopamine reward system.
In autism, attention is distributed differently — the system that decides how attention is allocated goes deep and narrow rather than broad and shallow, concentrating processing into fewer channels with greater intensity.
A growing body of research supports this distinction. Eye-tracking and EEG studies show that autistic attention is characterised by prolonged encoding, “sticky” disengagement, and a tendency to return to previous focuses — patterns that are measurably linked to sensory experience, perception, and learning12. Importantly, research also suggests that hyperfocus may involve fundamentally different processes in autism and ADHD, with measures of hyperfocus and flow being inversely related in ADHD adults12 — consistent with the idea that these are two distinct attentional differences, not the same one expressed differently.
In AuDHD, both are happening at once. Attention is distributed deeply and regulated by interest, which can produce the experience of wanting structure (because autistic depth of processing needs predictability) while simultaneously craving novelty (because ADHD regulation needs stimulation). Some interests persist for decades, held in place by the autistic distribution pattern. Others cycle rapidly through what the ADHD community calls the “hobby graveyard,” driven by the regulation pattern, chasing new stimulation.
The regulation-versus-distribution comparison is our own synthesis, not a framework that has been directly tested in a study. But both halves are individually well-supported, and we find it useful for understanding how the two conditions interact — and particularly for understanding why AuDHD is so often missed. The ADHD restlessness can look like social engagement, hiding the autistic social processing cost, while the autistic deep focus can look like sustained attention, hiding the ADHD regulation difficulty.
Articles on Autism
ADHD & Autism on the Rise: Are There More Neurodivergent People Now?
Why it seems there are more neurodivergent people now than before, when in fact we’ve always been here.
How to talk about neurodivergence in a kind way: terms & phrases to know
Talking about neurodivergence is not as clear-cut as it seems. The history of the treatment and acceptance of neurodivergent conditions is long and …
I Wasn’t ‘Just A Bit Stressed Out’
Exploring the impact of internalised ableism made me re-evaluate my misinterpreted autistic and ADHD traits.
Key terms to know
rigid thinking (cognitive inflexibility)
Cognitive inflexibility, also erroneously referred to as rigid thinking, is a diagnostic characteristic of autism that describes difficulty shifting between tasks, perspectives, or plans. The label captures how the trait looks from outside — but the internal experience is better understood through monotropism: a processing style that goes deep rather than wide. The depth that makes sustained …
restricted repetitive behaviours (RRBs)
Restricted Repetitive Behaviours (RRBs) is the clinical term for a broad group of autistic traits including stimming, echolalia, routines, persistent interests, and sensory sensitivities. Despite the pathologising name, these patterns serve real purposes — self-regulation, cognitive energy conservation, and genuine enjoyment. They are how an autistic nervous system manages a world that …
intolerance of uncertainty
Intolerance of uncertainty (IU) describes the degree to which a nervous system needs predictability in order to function — not as a preference, but as a genuine operational requirement. When outcomes are unknown or plans unconfirmed, a high-IU nervous system tends to generate contingencies: running through variables, gathering information in advance, and finding it difficult to settle until …
autistic burnout
Autistic burnout refers to a state of physical, mental, and emotional exhaustion experienced by autistic people. It is a result of prolonged exposure to overwhelming sensory, social, and cognitive demands, often in an environment that does not accommodate their needs.
masking
Masking is a partly unconscious effort to hide or suppress the manifestations of your neurodivergence. It is an exhausting process that many of us do to “fit in” more. Many people start to mask to avoid abuse, discrimination, bullying, harm and ableism.
double empathy
The double empathy problem is a concept in neurodiversity studies that suggests a mutual misunderstanding between neurodivergent and neurotypical individuals.

stimming
Stimming (self-stimulatory behaviour) tends to be more intense, deliberate, and repetitive. It can include hand flapping, rocking, making repetitive sounds, spinning, examining textures intensely, or listening to the same song on repeat for hours. Stimming is historically associated with autism and serves primarily as emotional and sensory regulation—a way to manage overwhelming feelings, …
context switching
Context switching refers to the cognitive process of shifting attention between different tasks or mental states. It involves disengaging from one task and engaging in another, requiring the brain to change its focus, rules, and objectives.
This process can be mentally taxing due to the cognitive …
pattern recognition in autism
Pattern recognition is a thinking style common in autistic people, involving a tendency to notice underlying structures, connections, and regularities across many areas of life — sensory, social, systemic, and practical. Research supports enhanced visual and perceptual pattern detection in …
literal thinking
Literal thinking is a precision-oriented processing style common in autistic people, where words, questions, and instructions are interpreted according to their exact meaning rather than their implied or intended meaning. It is one of the most commonly misunderstood autistic traits — both by …
special interests
Special interests are deeply focused areas of engagement that autistic people experience with a level of emotional investment, sustained attention, and joy that goes well beyond typical hobbies. Clinically categorised under restricted repetitive behaviours, special interests are one of the defining …
transitions
Transitioning, in the context of neurodiversity, refers to the process of moving from one state, activity, or place to another. It involves a shift in attention, focus, and cognitive resources.
For neurodivergent individuals, it may require additional time, support, and strategies to manage …
scripting
Scripting is a communication pattern where individuals use memorized or prepared phrases in their interactions. Common in autism, it serves as a valuable tool for managing social situations, expressing needs, and conserving energy while communicating. Scripting can be prepared ahead of time or drawn …
palilalia
Palilalia is a form of verbal expression where someone involuntarily repeats their own words or phrases, often with decreasing volume. This natural pattern can help with language processing and self-regulation, particularly during times of stress or when processing complex information.
hyperfixation
Hyperfixation is a term often used in the context of neurodivergent individuals, particularly Autistics and ADHDers. It refers to an intense and prolonged focus on a particular subject, topic, or activity, often at the price of excluding everything else.

executive dysfunction
Executive functions are essential, they help us make plans, stay organized, pay attention, and keep our emotions in check. It plays a big role in making decisions and adapting to new situations.
Executive dysfunction can happen when these processes have a difference or impairment that affects …
echolalia
Echolalia is a speech pattern where individuals repeat words, phrases, or sounds they have heard. Common in autism, it serves various purposes, including communication, language processing, and emotional expression. Echolalia can be immediate (repeating something just heard) or delayed (using stored …
demand avoidance
Demand avoidance means appearing opposed to doing something when it’s perceived as a demand, especially from an authority figure – even if you actually want to do the thing. While it may look like defiance or stubbornness to others, it’s actually an involuntary self-preservation response triggered …
ARFID
ARFID stands for Avoidant/Restrictive Food Intake Disorder. It is characterized by highly selective eating habits, often to the point of nutritional deficiency. Unlike anorexia or bulimia, ARFID is not driven by concerns about body image or weight. Instead, it’s typically related to sensory …
the mTOR pathway
The mTOR pathway is a signalling system inside every cell that regulates the balance between building new structures and recycling old ones. In autistic brains, this pathway runs hotter than typical, suppressing the cell’s internal cleanup processes. Up to 58% of autism-associated genes relate to …
synaptic pruning
Synaptic pruning is the process by which the brain refines its connections during development, removing synapses that are used less frequently while strengthening active ones. In autistic brains, this process works differently — two independent cleanup systems (the neuron’s internal recycling …

decompressing
Decompressing refers to engaging in activities or behaviours that allow a person to relax, unwind, and alleviate stress or sensory overload.
This term is particularly significant in the neurodivergent community as we often experience heightened sensitivity to environmental stimuli, leading to …
emotional dysregulation
Emotional dysregulation is the inability to regulate the intensity and quality of emotions in order to generate an appropriate emotional response and return to an emotional baseline.
When someone has difficulty regulating their emotions, they are easily overstimulated and they can get upset or …
verbal shutdown
Verbal shutdown is a temporary inability to produce speech despite having intact language and thoughts – an involuntary neurological response to overwhelm. It’s when words exist in one’s mind but cannot be physically spoken due to sensory, emotional, or cognitive overload.
Casually and incorrectly …

night terrors
Night terrors are episodes of intense fear during sleep that involve screaming, physical movement, and autonomic arousal (racing heart, rapid breathing, sweating). Unlike nightmares, they occur during non-REM sleep with no memory of the event afterwards.
Night terrors affect both children and …
penguin pebbling
In a neurodivergent context, the expression is used to describe a common neurodivergent behaviour of people collecting and giving loved items to others – “this made me think of you, I think you’ll like this, I thought this was pretty and I want you to have it”.
alexithymia
Alexithymia is the inability to assign names to feelings, describe them to others or talk about them. It is considered a separate neuropsychological condition but has significant overlaps with autism.

info dumping
Info dumping is the casual name referring to the act of sharing an extensive amount of information, usually about a subject or topic the person is extremely passionate about.
flat affect
Flat affect is an autistic speech pattern that can include fewer facial expressions, reduced eye contact and speech that others might describe as ‘monotone’. While these might be be interpreted as diminished emotional response, they actually reflect a different way of processing and expressing …
restriction
Restriction means being prevented from moving freely or being confined against your will. It can include being held down, trapped, or having your movement controlled by others. This is particularly important for neurodivergent people, who have historically faced harmful practices where restriction …
autistic speech patterns
Autistic speech patterns refer to unique ways autistic folks communicate or use language, but these patterns can also be present throughout the neurodivergent spectrum.
Autistic speech patterns include
– echolalia (echoing what you or others say),
– palilalia (repeating your own words or …
Autism questions, concerns, and wonderings — answered
“Why do I do better with a routine?”
Because routine is architecture you can rely on when everything else is wobbly or up in the air.
When you do the same things in the same order, your brain doesn’t have to build the day from scratch. The route is known, the sequence is mapped, all the decisions have already been made, and you are …
“Why do I watch the same show over and over?”
Because your nervous system is doing something smart, so good for you! 🙂
When you rewatch a familiar show, your brain isn’t processing anything new — no plot twists to manage, no unfamiliar characters to track, no sudden shifts in tone to adjust to.
“Is fidgeting and stimming the same thing?”
Fidgeting is similar to stimming, but they serve different purposes. While stimming tends to function as emotional regulation (a way to manage overwhelming feelings or sensory input), fidgeting more often serves focus regulation and energy discharge. The movements might look the same from the …

“I have tried traditional “self-care” activities, and they don’t do anything for me. What am I doing wrong?”
Nothing! Neurodivergent brains need more time to process, decompress, and recharge.
“I’m afraid of a diagnosis, I don’t want to be fixed!”
Good news: a neurodivergent diagnosis isn’t about fixing you, because you’re not broken. What it actually does is give you a framework to understand how your brain works and what you need – so you can finally stop forcing neurotypical solutions on yourself.

“What can a neurodivergent diagnosis give me if I got this far on my own?”
You’ve developed coping strategies and made it work so far. Hooray! But what’s working today might not work tomorrow — especially when life throws big changes at you like hormonal shifts, job changes, or major life transitions. A diagnosis can give you a baseline understanding …
“I don’t want to become my label and use my neurodivergence as an excuse”
If you’re worried about this, you’re already not that person. Asking for accommodations (like quiet spaces, reminders, breaks) is self-care and self-advocacy. The difference between advocating for your needs and being manipulative comes down to respect: are you communicating your limits while taking …
“Why get an ADHD / autism diagnosis just to get a label?”
Whether you like it or not, you already have labels — lazy, scatterbrain, weird, messy — given to you by others. You have probably internalised many of them over the decades, too. The difference with a diagnosis is that this label is one you choose for yourself based on understanding, …
What’s actually happening when I go into verbal shutdown?
A verbal shutdown might appear to be “nothing” from the outside, but actually, a lot is going on beneath the surface. Language, speech, even just on the technical side, are very complicated, even before you start adding the social layers on top of it (word choices, cadence, …
Research on Autism
This is the bibliography for all research that we used and cited on our website and informed our content on autism.
- "Attention Deficit Hyperactivity Disorder: Diagnosis and Management Guidance.” Nice.org.uk, NICE, 14 Mar. 2018, View source ↗ Discussed in: ADHD & Autism on the Rise: Are There More Neurodivergent People Now?
- Ingraham, Christopher. “The Surprising Geography of American Left-Handedness.” Washington Post, 22 Sept. 2015, View source ↗ Discussed in: ADHD & Autism on the Rise: Are There More Neurodivergent People Now?
- Xu, G., Strathearn, L., Liu, B., Yang, B., & Bao, W. (2018). Twenty-Year Trends in Diagnosed Attention-Deficit/Hyperactivity Disorder Among US Children and Adolescents, 1997-2016. JAMA network open, August 31, 2018. View source ↗ Discussed in: ADHD & Autism on the Rise: Are There More Neurodivergent People Now?
- Russell, Ginny, et al. “Time Trends in Autism Diagnosis over 20 Years: A UK Population‐Based Cohort Study.” Journal of Child Psychology and Psychiatry, vol. 63, no. 6, Aug. 2021, pp. 674–82, View source ↗ Discussed in: ADHD & Autism on the Rise: Are There More Neurodivergent People Now?
- Cameron, Sara. "Shark Attacks, Ice Creams, and the Randomised Trial". theGIST. November 12, 2018. [Accessed 15 Oct. 2024]. View source ↗ Discussed in: ADHD & Autism on the Rise: Are There More Neurodivergent People Now?
- Jeyshankar, R., & Vellaichamy, A., 2016. Scientometric Analysis of Autism Research Output during 2007-2011. SRELS Journal of Information Management, 53, pp. 55-63. View source ↗ Discussed in: ADHD & Autism on the Rise: Are There More Neurodivergent People Now?
- Shaw, M., Caci, H., Hodgkins, P., Kahle, J., Callamaras, N., & Woods, A., 2011. Long-term outcomes of ADHD: Global and regional study publication trends. European Psychiatry, 26, pp. 578 - 578. View source ↗ Discussed in: ADHD & Autism on the Rise: Are There More Neurodivergent People Now?
- Ghirardi, L., Brikell, I., Kuja-Halkola, R., Freitag, C. M., Franke, B., Asherson, P., Lichtenstein, P., & Larsson, H. (2018). The familial co-aggregation of ASD and ADHD: a register-based cohort study. Molecular Psychiatry, 23(2), 257-262. View source ↗ Discussed in: AuDHD
- Thapar, A. (2018). Discoveries on the genetics of ADHD in the 21st century: New findings and their implications. The American Journal of Psychiatry, 175(10), 943-950. View source ↗ Discussed in: AuDHD
- Dr. Service explains autistic burnout, how to stop it, how to recover, and how to prevent it YouTube View source ↗ Discussed in: autistic burnout
- Autistic burnout appears to be a phenomenon distinct from occupational burnout or clinical depression. View source ↗ Discussed in: autistic burnout
- Autistic Speech Patterns: Echolalia, Palilalia, Scripting, and Vocal Stimming NeuroDivergent Rebel's Substack View source ↗ Discussed in: autistic speech patterns
- Low Demand Parenting View source ↗ Discussed in: demand avoidance
- PDA Society UK View source ↗ Discussed in: demand avoidance
- Bethel, S. (2023, February 2). What is Echolalia? View source ↗ Discussed in: echolalia
- Stubblefield, H. (2016, October 28). Echolalia. View source ↗ Discussed in: echolalia
- Rudy, L. J. Why Does My Child With Autism Echo Words and Sounds? Verywell Health. View source ↗ Discussed in: echolalia
- Clark, C. A. (2019, June 6). Echolalia: When Children Repeat What You Say. Speech And Language Kids. View source ↗ Discussed in: echolalia
- Bennie, M. (2022, March 23). Understanding Echolalia in Autism Spectrum Disorders. Autism Awareness Centre. View source ↗ Discussed in: echolalia
- Cleveland Clinic (2023. October 17.) Echolalia. View source ↗ Discussed in: echolalia
- Lowry, L. (2018, October 29). 3 Things You Should Know About Echolalia View source ↗ Discussed in: echolalia
- McAllister, M., McFayden, T., & Harrop, C. (2025). Reports of Echolalia and Related Behaviors in Autism From Parents, Teachers, and Clinicians: Evidence From the Simon Simplex Collection.. Autism research : official journal of the International Society for Autism Research. View source ↗ Discussed in: echolalia
- Paulus, F. W., Ohmann, S., Möhler, E., Plener, P., & Popow, C. (2021). Emotional Dysregulation in Children and Adolescents With Psychiatric Disorders. A Narrative Review. Frontiers in Psychiatry, 12, 628252. View source ↗ Discussed in: emotional dysregulation
- Badgaiyan, R. D., Fischman, A. J., & Alpert, N. M. (2009). Dopamine Release During Human Emotional Processing. NeuroImage, 47(4), 2041. View source ↗ Discussed in: emotional dysregulation
- A Deeper Dive into Emotional Dysregulation and ADHD by Navdeep Vining B.A, M.C, Registered Provisional Psychologist Foothills Academy Society View source ↗ Discussed in: emotional dysregulation
- Arnsten, A. F. (2009). The Emerging Neurobiology of Attention Deficit Hyperactivity Disorder: The Key Role of the Prefrontal Association Cortex. The Journal of Pediatrics, 154(5), I. View source ↗ Discussed in: emotional dysregulation
- Pavlopoulou, G., Chandler, S., Lukito, S., Kakoulidou, M., Matejko, M., Jackson, I., Balwani, B., Boyens, T., Poulton, D., Harvey-Nguyen, L., Glen, Z., Wilson, A., Ly, E., Macauley, E., Hurry, J., Baker, S., & Sonuga-Barke, E. J. (2025). Situating emotion regulation in autism and ADHD through neurodivergent adolescents’ perspectives. Scientific Reports, 15(1), 37464. View source ↗ Discussed in: emotional dysregulation
- Children with ADHD have serious difficulties with EF in so many areas that some psychiatrists and psychologists have proposed renaming this disorder as EF disorder (Parker, 2011) or EF deficit disorder (Barkley, 2012). | Source View source ↗ Discussed in: executive dysfunction
- Carleton, R. N. (2016). Fear of the unknown: One fear to rule them all? Journal of Anxiety Disorders, 41, 5–21. View source ↗ Discussed in: intolerance of uncertainty
- Jenkinson, R., Milne, E., & Thompson, A. (2020). The relationship between intolerance of uncertainty and anxiety in autism: A systematic literature review and meta-analysis. Autism, 24(8), 1933–1944. View source ↗ Discussed in: intolerance of uncertainty
- Keefer, A., Singh, V., Jang, Y. S., Alon, L., Surmacz, M., Holingue, C., Mostofsky, S. H., & Vasa, R. A. (2024). Exploring the Symptom Profiles of Intolerance of Uncertainty in Autistic Children. Journal of autism and developmental disorders, 54(1), 121–130. View source ↗ Discussed in: intolerance of uncertainty
- Normansell-Mossa, K. M., et al. (2021). Sensory sensitivity and intolerance of uncertainty in autistic adults. Frontiers in Psychology, 12, 731753. View source ↗ Discussed in: intolerance of uncertainty
- Lennuyeux-Comnene, L., Yates, R., & Gaigg, S. B. (2024). What is uncertainty? A grounded theory of the role of uncertainty in anxiety in autism [Preprint]. Discussed in: intolerance of uncertainty
- Van de Cruys, S., Evers, K., Van der Hallen, R., Van Eylen, L., Boets, B., de-Wit, L., & Wagemans, J. (2014). Precise minds in uncertain worlds: Predictive coding in autism. Psychological Review, 121(4), 649–675. View source ↗ Discussed in: intolerance of uncertainty
- Dias, C., Sousa, T., Cruz, A., Costa, D., Mouga, S., Castelhano, J., Pires, G., & Castelo-Branco, M. (2025). A role for preparatory midfrontal theta in autism as revealed by a high executive load brain-computer interface reverse spelling task. Scientific reports, 15(1), 16671. View source ↗ Discussed in: intolerance of uncertainty
- Lacroix, A., Bennetot-Deveria, Y., Baciu, M., Dutheil, F., Magnon, V., Gomot, M., & Mermillod, M. (2024). Understanding cognitive flexibility in emotional evaluation in autistic males and females: the social context matters. Molecular autism, 15(1), 49. View source ↗ Discussed in: intolerance of uncertainty
- Mahmud F, Kang E, McDonald RG, Wallace D and Masia Warner C (2025) Disentangling the association between cognitive flexibility and anxiety in autistic youth: real-world flexibility versus performance-based task switching. Front. Psychiatry 16:1570185. Discussed in: intolerance of uncertainty
- Lage, C., Smith, E. S., & Lawson, R. P. (2024). A meta-analysis of cognitive flexibility in autism spectrum disorder. Neuroscience and biobehavioral reviews, 157, 105511. View source ↗ Discussed in: intolerance of uncertainty
- Benallie, K., et al. (2021). Executive functioning in children with ASD + ADHD and ASD + ID: A systematic review. Research in Autism Spectrum Disorders, Volume 86. View source ↗ Discussed in: intolerance of uncertainty
- Maisel, M. E., Stephenson, K. G., South, M., Rodgers, J., Freeston, M. H., & Gaigg, S. B. (2016). Modeling the cognitive mechanisms linking autism symptoms and anxiety in adults. Journal of Abnormal Psychology, 125(5), 692–703. View source ↗ Discussed in: intolerance of uncertainty
- Lin, Y., Mason, D., Hirsch, C., & Happé, F. (2025). Intolerance of Uncertainty and Anxiety (but not Alexithymia) Mediate the Association Between Autistic Traits and Quality of Life. Journal of autism and developmental disorders, 55(4), 1389–1401. View source ↗ Discussed in: intolerance of uncertainty
- Bird, G., et al. (2024). Anxiety, intolerance of uncertainty and restricted and repetitive behaviours in autism spectrum disorder: A systematic review and meta-analysis. Research in Autism Spectrum Disorders, Volume 117, 2024 View source ↗ Discussed in: intolerance of uncertainty
- Joyce, C., Honey, E., Leekam, S. R., Barrett, S. L., & Rodgers, J. (2017). Anxiety, Intolerance of Uncertainty and Restricted and Repetitive Behaviour: Insights Directly from Young People with ASD. Journal of autism and developmental disorders, 47(12), 3789–3802. Journal of autism and developmental disorders, 47(12), 3789–3802. View source ↗ Discussed in: intolerance of uncertainty
- Skaletski, E. C., Bradley, L., Taylor, D., Travers, B. G., & Bishop, L. (2021). Quality-of-life discrepancies among autistic adolescents and adults: A rapid review. American Journal of Occupational Therapy, 75(3), 7503180090. View source ↗ Discussed in: intolerance of uncertainty
- Milton, D. E. M. (2012). On the ontological status of autism: the ‘double empathy problem.’ Disability & Society, 27(6), 883–887. View source ↗ Discussed in: intolerance of uncertainty
- O'Shea, A., Cersosimo, R., & Engelhardt, P. E. (2026). Online Metaphor Comprehension in Adults with Autism Spectrum Disorders: An Eye Tracking Study. Journal of autism and developmental disorders, 56(1), 56–70. View source ↗ Discussed in: literal thinking
- Lampri, S., Peristeri, E., Marinis, T., & Andreou, M. (2024). Figurative language processing in autism spectrum disorders: A review. Autism research : official journal of the International Society for Autism Research, 17(4), 674–689. View source ↗ Discussed in: literal thinking
- Deliens, G., Papastamou, F., Ruytenbeek, N., Geelhand, P., & Kissine, M. (2018). Selective Pragmatic Impairment in Autism Spectrum Disorder: Indirect Requests Versus Irony. Journal of autism and developmental disorders, 48(9), 2938–2952. View source ↗ Discussed in: literal thinking
- Leung, A., Leung, A., Wong, A., & Hon, K. (2020). Sleep Terrors: An Updated Review. Current Pediatric Reviews, 16, 176 - 182. View source ↗ Discussed in: night terrors
- 38% of children had night terrors; sleep issues linked to ADHD subtype. Chiang, H., Gau, S., Ni, H., Chiu, Y., Shang, C., Wu, Y., Lin, L., Tai, Y., & Soong, W. (2010). Association between symptoms and subtypes of attention‐deficit hyperactivity disorder and sleep problems/disorders. Journal of Sleep Research, 19. View source ↗ Discussed in: night terrors
- A comprehensive analysis of 47 studies revealing significantly higher prevalence of parasomnias, including night terrors, in autistic children compared to neurotypical peers. Feng, S., Huang, H., Wang, N., Wei, Y., Liu, Y., & Qin, D. (2021). Sleep Disorders in Children With Autism Spectrum Disorder: Insights From Animal Models, Especially Non-human Primate Model. Frontiers in behavioral neuroscience, 15, 673372. View source ↗ Discussed in: night terrors
- Hvolby A. (2015). Associations of sleep disturbance with ADHD: implications for treatment. Attention deficit and hyperactivity disorders, 7(1), 1–18. View source ↗ Discussed in: night terrors
- Coogan, A., & McGowan, N. (2017). A systematic review of circadian function, chronotype and chronotherapy in attention deficit hyperactivity disorder. ADHD Attention Deficit and Hyperactivity Disorders, 9, 129-147. View source ↗ Discussed in: night terrors
- Symptoms include mood swings, irritability, anxiety, fatigue, physical discomfort, and disruptions to sleep and circadian rhythms, such as altered melatonin secretion. Meth, E., Nôga, D., Dubol, M., Xue, P., Sundström-Poromaa, I., & Benedict, C. (2025). The impact of pharmacotherapy for premenstrual dysphoric disorder on sleep.. Sleep medicine reviews, 80, 102069 . https://doi.org/10.1016/j.smrv.2025.102069. View source ↗ Discussed in: night terrors
- Rivera, L. (2023): Autistic Speech Patterns: Echolalia, Palilalia, Scripting, and Vocal Stimming View source ↗ Discussed in: palilalia
- Arps, K. (2025): Palilalia View source ↗ Discussed in: palilalia
- McClure, C. (2024): Yes, Yes! How Repeating Words (Palilalia) Achieves Better Language Processing View source ↗ Discussed in: palilalia
- Evers, K., Hallen, R., Noens, I., & Wagemans, J. (2018). Perceptual organization in individuals with autism spectrum disorder. Child Development Perspectives, 12(3), 177–182. Discussed in: pattern recognition in autism
- Samson, F., Mottron, L., Soulières, I., & Zeffiro, T. (2012). Enhanced visual functioning in autism: An ALE meta-analysis. Human Brain Mapping, 33(7), 1553–1581. Discussed in: pattern recognition in autism
- Crespi, B. (2021). Pattern unifies autism. Frontiers in Psychiatry, 12, 621659. Discussed in: pattern recognition in autism
- Roels, S., Begeer, S., Scheeren, A., & Van Prooijen, J. (2024). Conspiracy mentality in autistic and non-autistic individuals. Cognitive Neuropsychiatry, 29, 228–241. Discussed in: pattern recognition in autism
- Blain, S., Longenecker, J., Grazioplene, R., Klimes-Dougan, B., & DeYoung, C. (2020). Apophenia as the disposition to false positives: A unifying framework for openness and psychoticism. Journal of Abnormal Psychology, 129(3), 279–292. Discussed in: pattern recognition in autism
- Bennert, K., Brosnan, M., Canning, A., Roberts, G., & Russell, A. (2024). Paranoia and data-gathering biases in autism. Journal of Autism and Developmental Disorders, 55, 1402–1410. Discussed in: pattern recognition in autism
- Georgiou, N., Balzan, R., Delfabbro, P., & Young, R. (2024). People with autistic traits are more likely to engage with misinformation and conspiracy theories in a simulated social media context. Cognitive Neuropsychiatry, 29, 286–305. Discussed in: pattern recognition in autism
- Collis, E., Gavin, J., Russell, A., & Brosnan, M. (2022). Autistic adults' experience of restricted repetitive behaviours. Research in Autism Spectrum Disorders, 90, 101895. Discussed in: restricted repetitive behaviours (RRBs)
- Kapp, S. K., Steward, R., Crane, L., Elliott, D., Elphick, C., Pellicano, E., & Russell, G. (2019). 'People should be allowed to do what they like': Autistic adults' views and experiences of stimming. Autism, 23(7), 1782–1792. Discussed in: restricted repetitive behaviours (RRBs)
- Collis, E., Dark, E., Russell, A., & Brosnan, M. (2024). Self-report of restricted repetitive behaviours in autistic adults: A systematic review. Autism in Adulthood. Discussed in: restricted repetitive behaviours (RRBs)
- Masjedi, N., Clarke, E. B., & Lord, C. (2024). Development of restricted and repetitive behaviors from 2–19: Stability and change in repetitive sensorimotor, insistence on sameness, and verbal behaviors in a longitudinal study of autism. Journal of Autism and Developmental Disorders. Discussed in: restricted repetitive behaviours (RRBs)
- Nwaordu, G., Charlton, R.A. Repetitive Behaviours in Autistic and Non-Autistic Adults: Associations with Sensory Sensitivity and Impact on Self-Efficacy. J Autism Dev Disord 54, 4081–4090 (2024). View source ↗ Discussed in: restricted repetitive behaviours (RRBs)
- Anderson, K. (2022, November 15th) Echolalia and Scripting: Supporting Autistic Rights and Fighting Speech Stigma. View source ↗ Discussed in: scripting
- Sullivan, D. (2020, April 9th.) Echolalia and Scripting in Autism: Why We Autistics Repeat View source ↗ Discussed in: scripting
- O'Connor, S. (2022) What Is Autistic Scripting? View source ↗ Discussed in: scripting
- Long, R. (2024). Access Points: Understanding Special Interests Through Autistic Narratives. Autism in Adulthood, 7, 100–111. View source ↗ Discussed in: special interests
- Grove, R., Hoekstra, R.A., Wierda, M., & Begeer, S. (2018). Special interests and subjective wellbeing in autistic adults. Autism Research, 11. View source ↗ Discussed in: special interests
- Bross, L., Huffman, J., & Hagiwara, M. (2022). Examining the special interest areas of autistic adults with a focus on their employment and mental health outcomes. Journal of Vocational Rehabilitation, 57, 289–305. View source ↗ Discussed in: special interests
- Murray, D., Lesser, M., & Lawson, W. (2005). Attention, monotropism and the diagnostic criteria for autism. Autism, 9(2), 139–156. View source ↗ Discussed in: special interests
- Clements, C.C., Zoltowski, A.R., Yankowitz, L.D., Yerys, B.E., Schultz, R.T., & Herrington, J.D. (2018). Evaluation of the Social Motivation Hypothesis of Autism: A Systematic Review and Meta-analysis. JAMA Psychiatry, 75(8), 797–808. View source ↗ Discussed in: special interests
- Kohls, G., Schulte-Rüther, M., Nehrkorn, B., Müller, K., Fink, G.R., Kamp-Becker, I., Herpertz-Dahlmann, B., Schultz, R.T., & Konrad, K. (2013). Reward system dysfunction in autism spectrum disorders. Social Cognitive and Affective Neuroscience, 8(5), 565–572. View source ↗ Discussed in: special interests
- Caldwell-Harris, C., & Jordan, C. (2013). Systemizing and special interests: Characterizing the continuum from neurotypical to autism spectrum disorder. Learning and Individual Differences, 29, 98–105. View source ↗ Discussed in: special interests
- Edwards, H., Wright, S., Sargeant, C., Cortese, S., & Wood-Downie, H. (2023). Research Review: A systematic review and meta-analysis of sex differences in narrow constructs of restricted and repetitive behaviours and interests in autistic children, adolescents, and adults. Journal of Child Psychology and Psychiatry. View source ↗ Discussed in: special interests
- Putnam, O.C., Swisher, M., McFayden, T., Chan, D., & Harrop, C. (2025). The Role of Gender and Strong Interests in Self-Reported Camouflaging of Autistic Adults. Neurodiversity, 3. View source ↗ Discussed in: special interests
- Evans, J.A., Krumrei-Mancuso, E.J., & Rouse, S.V. (2023). What You Are Hiding Could Be Hurting You: Autistic Masking in Relation to Mental Health, Interpersonal Trauma, Authenticity, and Self-Esteem. Autism in Adulthood, 6, 229–240. View source ↗ Discussed in: special interests
- Harrop, C., Amsbary, J., Towner-Wright, S., Reichow, B., & Boyd, B.A. (2019). That's what I like: The use of circumscribed interests within interventions for individuals with autism spectrum disorder. A systematic review. Research in Autism Spectrum Disorders. View source ↗ Discussed in: special interests
- Pathophysiology of tics and Tourette syndrome A. Berardelli, et. al. (2003) View source ↗ Discussed in: stimming
- Sakai, J. (2020). Core Concept: How synaptic pruning shapes neural wiring during development and, possibly, in disease. Proceedings of the National Academy of Sciences, 117, 16096–16099. https://doi.org/10.1073/pnas.2010281117 Discussed in: synaptic pruning
- Faust, T., Gunner, G., & Schafer, D. (2021). Mechanisms governing activity-dependent synaptic pruning in the developing mammalian CNS. Nature Reviews Neuroscience, 22, 657–673. https://doi.org/10.1038/s41583-021-00507-y Discussed in: synaptic pruning
- Neniskyte, U., & Gross, C. (2017). Errant gardeners: glial-cell-dependent synaptic pruning and neurodevelopmental disorders. Nature Reviews Neuroscience, 18, 658–670. https://doi.org/10.1038/nrn.2017.110 Discussed in: synaptic pruning
- Tang, G., Gudsnuk, K., Kuo, S., et al. (2014). Loss of mTOR-Dependent Macroautophagy Causes Autistic-like Synaptic Pruning Deficits. Neuron, 83, 1131–1143. https://doi.org/10.1016/j.neuron.2014.07.040 Discussed in: synaptic pruning
- Kim, H., et al. (2016). Deficient autophagy in microglia impairs synaptic pruning and causes social behavioral defects. Molecular Psychiatry, 22, 1576–1584. https://doi.org/10.1038/mp.2016.103 Discussed in: synaptic pruning
- Pagani, M., et al. (2021). mTOR-related synaptic pathology causes autism spectrum disorder-associated functional hyperconnectivity. Nature Communications, 12. https://doi.org/10.1038/s41467-021-26131-z Discussed in: synaptic pruning
- Westacott, L., & Wilkinson, L. (2022). Complement Dependent Synaptic Reorganisation During Critical Periods of Brain Development and Risk for Psychiatric Disorder. Frontiers in Neuroscience, 16. https://doi.org/10.3389/fnins.2022.840266 Discussed in: synaptic pruning
- Müller, R., et al. (2011). Underconnected, but how? A survey of functional connectivity MRI studies in autism spectrum disorders. Cerebral Cortex, 21(10), 2233–2243. https://doi.org/10.1093/cercor/bhq296 Discussed in: synaptic pruning
- Silva, P. (2018). Do patterns of synaptic pruning underlie psychoses, autism and ADHD? BJPsych Advances, 24, 212–217. https://doi.org/10.1192/bja.2017.27 Discussed in: synaptic pruning
- Hay, N., & Sonenberg, N. (2004). Upstream and downstream of mTOR. Genes & Development, 18, 1926–1945. https://doi.org/10.1101/gad.1212704 Discussed in: the mTOR pathway
- Tang, G., Gudsnuk, K., Kuo, S., et al. (2014). Loss of mTOR-Dependent Macroautophagy Causes Autistic-like Synaptic Pruning Deficits. Neuron, 83, 1131–1143. https://doi.org/10.1016/j.neuron.2014.07.040 Discussed in: the mTOR pathway
- Trifonova, E.A., et al. (2021). Do Autism Spectrum and Autoimmune Disorders Share Predisposition Gene Signature Due to mTOR Signaling Pathway Controlling Expression? International Journal of Molecular Sciences, 22(10), 5248. https://doi.org/10.3390/ijms22105248; Winden, K.D., Ebrahimi-Fakhari, D., & Sahin, M. (2018). Abnormal mTOR Activation in Autism. Annual Review of Neuroscience, 41, 1–23. https://doi.org/10.1146/annurev-neuro-080317-061747 Discussed in: the mTOR pathway
- Sahin, M., & Sur, M. (2015). Genes, circuits, and precision therapies for autism and related neurodevelopmental disorders. Science, 350(6263). https://doi.org/10.1126/science.aab3897; Parenti, I., Rabaneda, L., Schoen, H., & Novarino, G. (2020). Neurodevelopmental Disorders: From Genetics to Functional Pathways. Trends in Neurosciences, 43, 608–621. https://doi.org/10.1016/j.tins.2020.05.004 Discussed in: the mTOR pathway
- Bozzi, Y., Provenzano, G., & Casarosa, S. (2018). Neurobiological bases of autism-epilepsy comorbidity: a focus on excitation/inhibition imbalance. European Journal of Neuroscience, 47(6), 534–548. https://doi.org/10.1111/ejn.13595 Discussed in: the mTOR pathway
- Pagani, M., et al. (2021). mTOR-related synaptic pathology causes autism spectrum disorder-associated functional hyperconnectivity. Nature Communications, 12. https://doi.org/10.1038/s41467-021-26131-z Discussed in: the mTOR pathway
- Wang, L., et al. (2022). mTOR Signaling Pathway Regulates the Release of Proinflammatory Molecule CCL5 Implicated in the Pathogenesis of Autism Spectrum Disorder. Frontiers in Immunology, 13, 818518. https://doi.org/10.3389/fimmu.2022.818518 Discussed in: the mTOR pathway
- Ye, X., et al. (2020). Lipopolysaccharide induces neuroinflammation in microglia by activating the MTOR pathway and downregulating Vps34 to inhibit autophagosome formation. Journal of Neuroinflammation, 17, 18. https://doi.org/10.1186/s12974-019-1644-8 Discussed in: the mTOR pathway
- Hsieh, C. (2023). "Going Nonverbal Doesn't Mean What You Think It Means" View source ↗ Discussed in: verbal shutdown
- Dr. Bercovici, PhD (2023) "Selective mutism & autism" View source ↗ Discussed in: verbal shutdown
- Kaelynn Partlow on Instagram View source ↗ Discussed in: verbal shutdown
- Riggs, C. (2021) "Ask the Expert: 'Nonspeaking' vs. 'Nonverbal' and Why Language Matters" View source ↗ Discussed in: verbal shutdown
- Nonspeaking Autistic Students Resources View source ↗ Discussed in: verbal shutdown
- Nonspeaking from Stimpunks Foundation View source ↗ Discussed in: verbal shutdown
